SARS-CoV-2 which is the causative agent for COVID-19 pandemic continues to manifest with severe acute respiratory syndrome among the adults and slowly afflicting the human race. The patients require ICU facility, artificial ventilation and sometimes extracorporeal membrane oxygenation. The hospitals of several countries are overloaded with such ICU patients for treatment. This evocative scenario of COVID-19 pandemic has presented a formidable defiance even for most sophisticated hospital settings. Under such pressing circumstances multidrug resistant human fungus, Candida auris represents a rising challenge not receiving due considerations by majority of health professionals.
Identified in 2009, C. auris is now recognized as an emerging species of concern. C. auris is recognized as a newly emerging species that was first identified from the ear canal of a patient in Japan. This human pathogen is associated with severe invasive infections with high mortality rates ranging from 40 to 72 %. C. auris has been recognized as globally emerging multidrug resistant fungal pathogen. Since June 2016, government institutions (CDC, WHO, NICD) issued clinical alert to health care facilities and provided interim guidelines for clinical management, laboratory testing and infection control. The emergence of C. auris in India was noted in sporadic outbreaks in a multicentric study of candidemia among Intensive Care Units in 2011. C. auris is posing significant challenges to microbiologists and clinicians because of its a) frequent multidrug resistance which is a norm rather exception; b) high transmissibility in hospital settings and severe outcomes; c) misidentification by standard biochemical identification systems. Moreover, the widespread and prolonged use of available antifungal drugs has given rise to multidrug resistance that alters the therapeutic available options. It has been reported that nearly 90% of C. auris isolates exhibit resistance to fluconazole, nearly 30% resistance to amphotericin B, and less than 5% resistance to echinocandins. Thus intrinsic drug resistance and lack of effective treatment strategies suggested that C. auris has all the features of a “superbug”. To make the matter worse, with the increment in SARS-Cov-2 infected patients, most of the hospital settings will serve as conducive environment for C. auris transmission because of its ability to persist on the surfaces and a known environmental colonizer of ICUs.
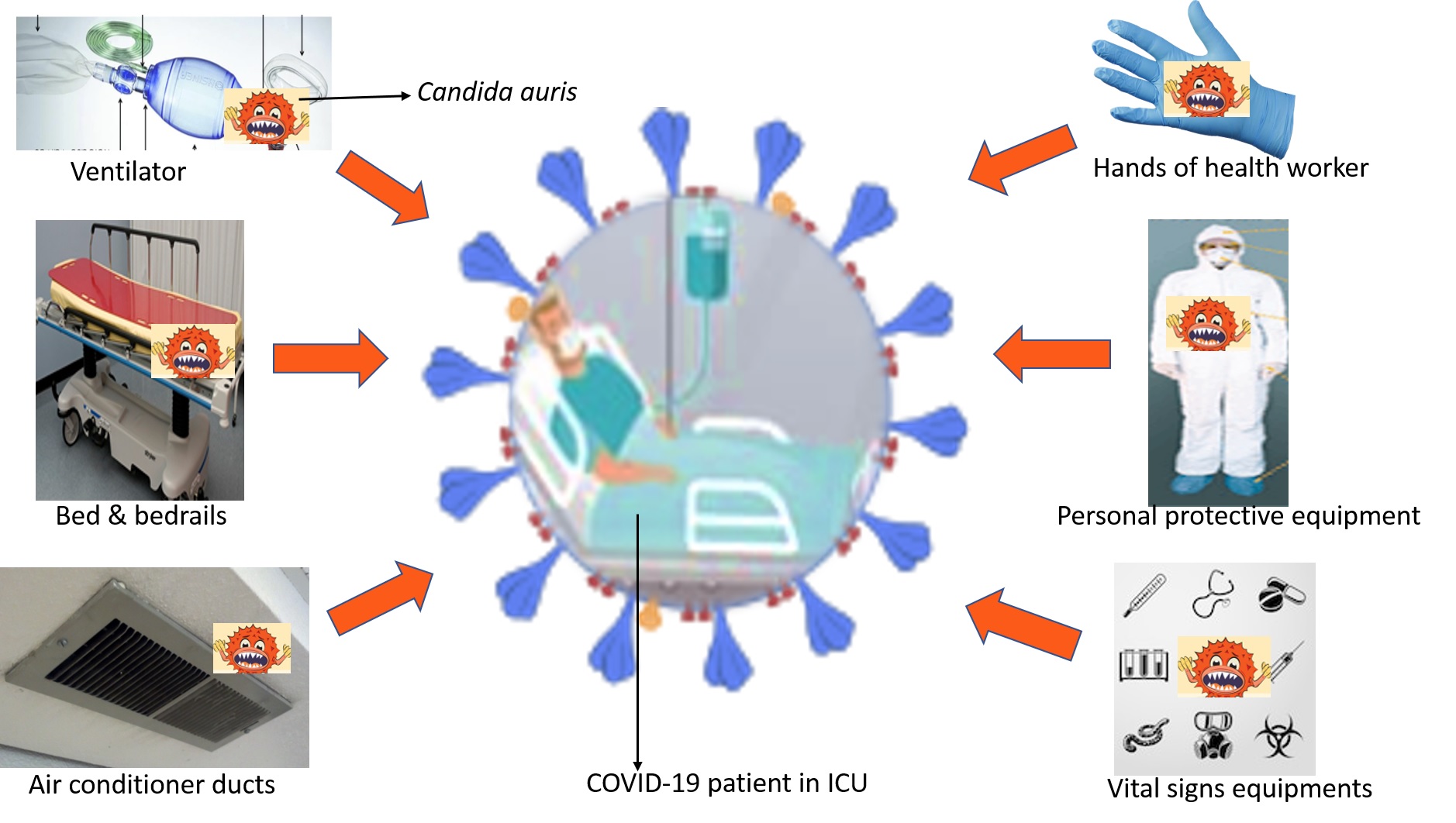
Similar to SARS-CoV-2, C. auris and has been found on hospital surfaces including on bedrails, beds, air conditioner ducts, windows and hospital floors. Unlike other Candida spp, C. auris has ability to reside on surfaces and therefore patients themselves are viable sources of shedding yeast cells from their skin and contaminate hospital environments. C. auris has all the properties to thrive and disseminate in such conditions. Infact, COVID-19 patients tends to share common risk factors with C. auris. Hence the standard procedures adopted for the management of COVID-19 critical care will make these patients more susceptible to colonization and infections by C. auris. The developing countries have more severe challenge such as over-loaded beds and less stringent infection control practices. The COVID-19 patients pre-colonized with C. auris and having the requirement of catheters will be at higher risk of developing C. auris infections in ICU.
The diagnostics of C. auris infections itself is a challenging task hence awareness and alertness of medical community for C. auris amidst this ongoing pandemic is a necessity. Since much of the focus nowadays is diverted towards the diagnosis and treatment of Sars-Cov-2 hence it is quite possible that the diagnosis of pathogens such as C. auris may be ignored or not paid due attention. This could lead to possible outbreaks of C. auris infections particularly in developing nations. Infact the mortality associated with COVID-19 pandemic also having contributions from C. auris or other such infections cannot be ruled out. The strict isolation of C. auris infected patient according to CDC, USA guidelines may not be implemented during the COVID-19 pandemic when health professionals are overburdened, remains a thought provoking issue. Hence strict surveillance on C. auris even during the times of COVID-19 pandemic is warranted globally.